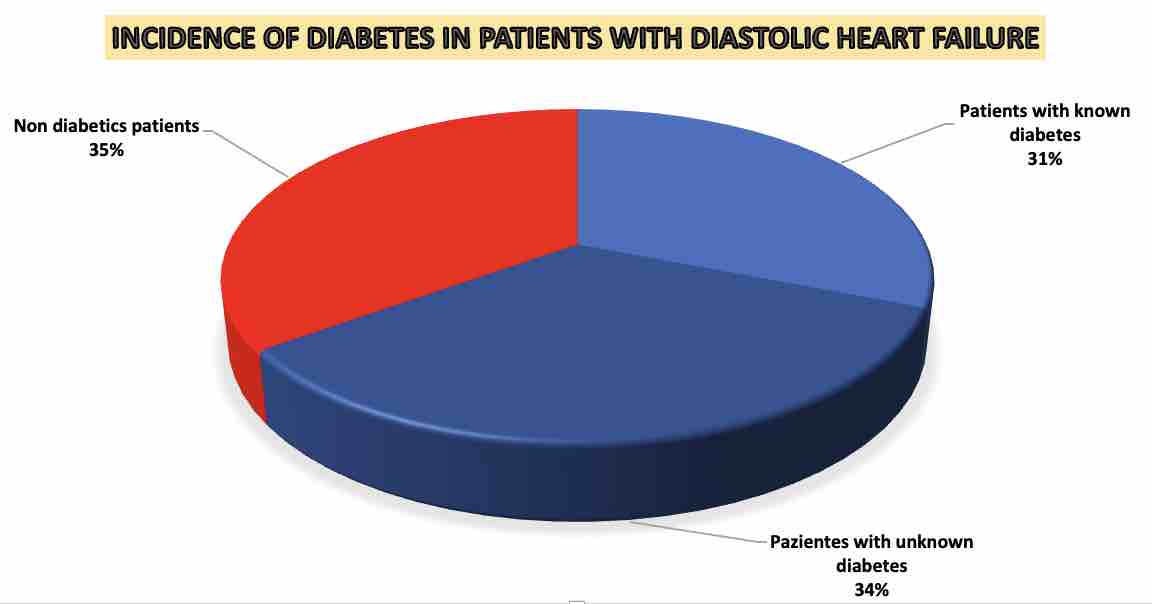
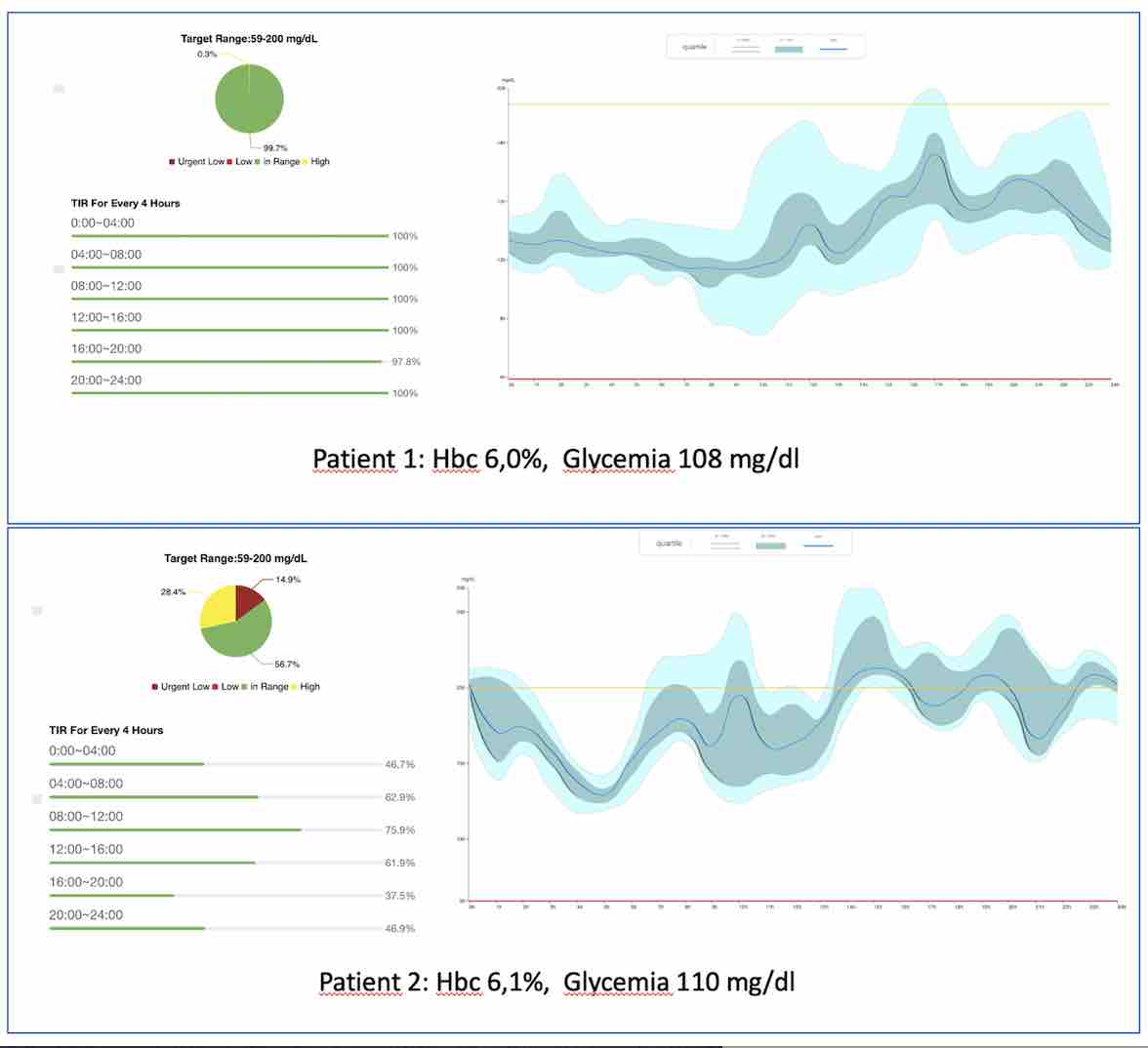
Background: Recently the guidelines of EACP reported a prevalence of diabetes mellitus in patients with diastolic heart failure (HFpEF) of 31%.Glunovo® is a transdermal device capable of detecting and storing the concentration of glucose in the abdominal interstitial fluid 480 times a day for up to 14 consecutive days. It is a new generation system for the continuous monitoring of glucose. Pourpose: In this study we used Glunovo® to evaluate the glycaemic variability in HFpEFMETHODS: 100 patients with HFpEF admitted to 4 Italian centres were enrolled consecutively. Glunovo® was applied to each enrolled patient for 7 days, taking a total of 3360 punctual glucose measurements for each patient in the abdominal interstitial fluid. Inclusion criteria: signs or symptoms of congestive heart failure; left ventricular function >55%; abnormal relaxation pattern of transmitral flow and an increased E/E’ ratio in tissue doppler of lateral left ventricular wall. We calculated for each patient the glycaemic variability and the incidence of hyperglycaemia and hypoglycaemia. Overall, 43 males and 57 females were enrolled with a mean age of 69.3 years (39-87 years). Results: In 94 of the 100 patients enrolled it was possible to conclude the analysis. A glycaemia >=200 mg/dL was found in 53 patients (56%) while a high glycaemic variability was found in 51 patients (54%). A blood glucose value <59 mg/dl was found in 48 patients (51%). Only 5 times the estimated glycated Hb values were> 6.5%. 32 of the patients with glycemic variability performed an oral glucose load curve, that in all cases confirmed the diabete. No statistically significant differences were found based on age group or sex. A control group of 10 patients without HFpEF was tested with Glunovo® and a glycaemic variability in only 1 patient (10%). Conclusion: Our experience suggests an incidence of hyperglycaemia and glycaemic variability more then 65% in patients affected by HFpEF. If our data were reproducible on a large scale, a so high prevalence of diabetes in patients with HFpEF cold explain the efficacy of SGLT-2 inhibitor and GLP-1 Agonist in this class of patients. Figure 1: Graphical reproduction of the glycaemic trend in two different patients with similar HBA1c and similar fast plasma glucose. Figure 2: Graphical reproduction of the estimated incidence of diabetes based on our analysis.